Nebadita is experienced in the field of nutrition, health, fitness, and more. Nebadita earned Master Degree from National Institute of Nutrition, Hyderabad and currently serving in the Eastern branch of ICMR. Know More. Learn about our editorial process.
The pregnant adolescent is more likely to be a member of a poor or low- family (83%), to be unmarried (72%), and to have an unplanned pregnancy (90%).
A proper assessment can identify individuals who are significantly underweight or overweight as well as those with conditions such as bulimia, anorexia, pica, hypovitaminosis, or hypervitaminosis and special dietary habits, such as vegetarianism.
Out of these, 51% end in live births, 35% end in induced abortion, and 14% result in a miscarriage or stillbirth.
Importance of nutrition during pregnancy is very important for a healthy baby. Proper nutrition during pregnancy and the nutritional support a mother and her developing fetus begins before conception. This poses a challenge for pediatricians caring for pregnant adolescents. Approximately 1 million teenagers become pregnant in the United States each year. Out of these, 51% end in live births, 35% end in induced abortion, and 14% result in a miscarriage or stillbirth.
Although birth rates to adolescents decreased in the 1990’s, the teenage birth rate in 1996 (54.7 live births/ 1000) was still higher than the rate in 1980. The pregnant adolescent is more likely to be a member of a poor or low- family (83%), to be unmarried (72%), and to have an unplanned pregnancy (90%).
One third of adolescents who become parents—mothers as well as fathers—were themselves the product of an adolescent pregnancy. Recent report showed more decreased in the teenage birth rate in 2019 (41.57 live births/1000) world-wide.(1)
Adolescent pregnancy is associated with an increased risk of medical complications, such as low birth weight, neonatal death, maternal mortality pregnancy-induced hypertension, and sexually transmitted infections: the youngest adolescents appear to be at greatest risk.
A low pre-pregnancy body mass index (BMI), low gestational weight gain, anemia, and a poor-quality diet are related to poor pregnancy outcomes among adolescents. So, a good nutrition during pregnancy is very important.
Early prenatal care, including assessment of nutritional status, is of paramount importance for pregnant adolescents.
A proper assessment can identify individuals who are significantly underweight or overweight as well as those with conditions such as bulimia, anorexia, pica, hypovitaminosis, or hypervitaminosis and special dietary habits, such as vegetarianism. However, due to the poor nutrition during pregnancy effects on the baby.
Assessment of Nutritional Status.
Due to poor nutrition during pregnancy, underweight women are at increased risk of reproductive problems. Not only fertility is compromised, but also, the likelihood of preterm delivery and intrauterine growth restriction (IUGR) is increased.
In addition, Apgar scores of offspring of underweight women are more frequently low. The condition of being underweight is potentially modifiable, because it is often related to unhealthy nutrition plan or exercise programs during pregnancy.
A woman motivated toward increasing her body weight according to the height may achieve her goal within a relatively short period (3 to 6 months).
Overweight women are at greater risk than normal-weight women for an unsatisfactory course or outcome of pregnancy.
Numerous studies have shown that obese women are at higher risk of prenatal complications, such as gestational diabetes, infertility, hypertension, and pyelonephritis.
They are also likely to experience prolonged labor followed by difficult vaginal delivery and thus, more frequently deliver by cesarean section. The incidence of adverse perinatal outcomes is likewise higher.
The weight of woman planning to become pregnant may be evaluated by her pre-pregnancy BMI, defined as weight (in kg) divided by height in meter square.
Table 1: Classification of Adult Maternal Pre-pregnancy Body Mass Index (BMI)
Classification
BMI
Underweight
<19.8
Normal Weight
19.8-26.0
Overweight
>26.0-29.0
Obese
>29.0
During adolescence, the categories weight in table are referenced by percentiles because of continued linear growth during those years.
Substantial evidence indicates that optimal birth weight is influenced by gestational weight gain. Methodologically acceptable studies have been virtually unanimous in reporting a positive relationship between birth weight and gestational weight gain.
However, maternal pre-pregnancy BMI is a strong effect modifier of this relationship. A number of studies have demonstrated an increased risk of IUGR with low total gestational weight gain.
Others have observed a specific risk associated with low weight gain during the second trimester and/or the third trimester of pregnancy.
On other hand, the increased risk of having large-for-gestational-age infants is associated with excessive gestational weight gain in very obese (BMI >35) women.
Obese women are more likely to have pregnancy complications of diabetes, hypertension, pre-eclampsia, arrest of labor, fetal distress and cesarean delivery.
The recognized relationship between gestational weight gain and birth weight underlies the 1990 Institute of Medicine (IOM) recommendations for weight gain on the basis of pre-pregnancy BMI.
Weight gain associated with optimal birth weights and least neonatal morbidity were determined. Recommended ranges for gestational weight gain by pre-pregnancy BMI are shown in Table 2.
Table 2: Recommended Total Gestational Weight Gain Ranges for Pregnant Women by Pre-pregnancy BMI.
Pre-pregnancy BMI
Recommended Gestational Weight Gain
Underweight (<19.8)
12.5-18 kg (28-40 lb)
Normal Weight (19.8-26.0)
11.5-16 kg (25-35 lb)
Overweight (>26.0-29.0)
7-11.5 kg (15-25 lb)
Obese (>29.0)
At least 6 kg (at least 15 lb)
What Nutrients Need to be Increased During Pregnancy.
It is important to plan a balanced and proper nutrition during pregnancy. As it can support a women and her baby during such crucial time. Here are some nutrition needs during pregnancy;
Energy.
Energy requirements during pregnancy increase as a result of increases in basal and activity energy expenditure and energy deposition in the newly acquired fetal and maternal tissues.
Obligatory energy needs of the fetus, uterus, placenta, and mammary glands have been estimated to represent only 15%, of the total requirement; the remainder supports energy needs for maintenance, work, and maternal fat deposition.
Basal energy expenditure increases during pregnancy as a result of the metabolic contribution of the uterus and fetus and increased work of the heart, lungs, and kidney.
The increased basal metabolic rate (BMR) is one of the major components of the increased energy requirement during pregnancy.
Variation in energy expenditure between Individuals is largely attributable to differences in fat-free mass, which in pregnancy comprises the expanded plasma, high-energy-requiring fetal and uterine tissues, and moderate- energy-requiring skeletal muscle mass.
In late pregnancy, approximately half of the increment in basal energy expenditure can be attributed to the fetus.
BMR of pregnant women has been measured longitudinally in a number of studies using a Douglas bag, ventilated hood, or whole-body respiration calorimeter. An additional 350kcal should be given in the daily diet.
Until late gestation, the gross energy cost of standardized non-weight-bearing activity does not significantly change. In the last month of pregnancy, the gross energy cost of cycling was increased on the order of 10%.
The energy cost of standardized weight-bearing activities, such as treadmill walking, was unchanged until 25 weeks of gestation, after which it is increased by 19%.
Standardized protocols, however, do not allow for behavioral changes in pace and intensity of physical activity, which may occur and conserve energy during pregnancy.
The doubly labeled water method has been used in 5 studies of well-nourished, pregnant women to measure free living total energy expenditure (TEE). TEE increased from approximately 2200 to 2400 kcal/day before pregnancy to 2700 kcal/day in the third trimester.
Activity energy expenditure or physical activity level decreased by the 36th week of gestation, compared with levels before expenditure.
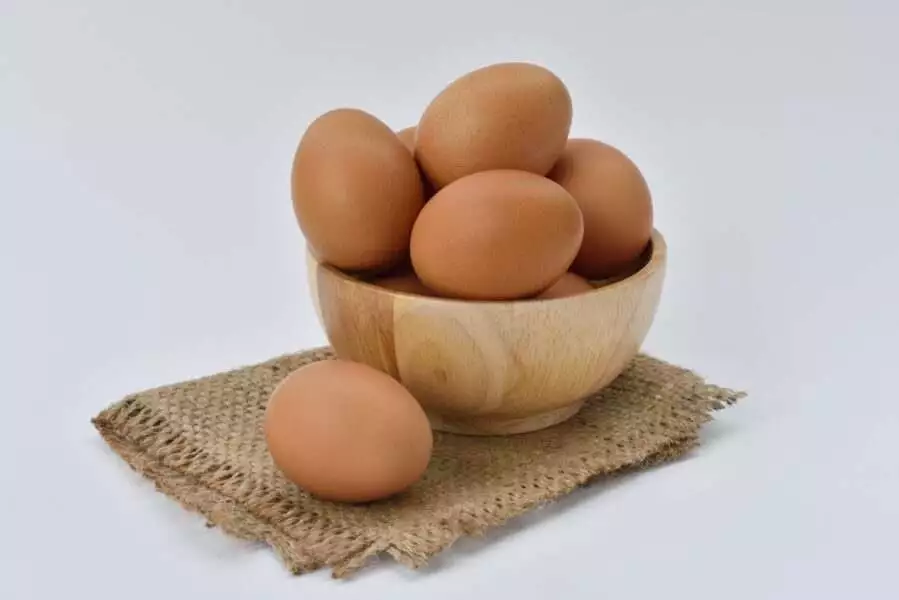
Protein requirements increase during pregnancy as a result of the increase in protein turnover and protein deposition in the Fetus, uterus, expanded maternal blood volume, mammary glands, and skeletal muscle. So, it is consider as one of the best nutrition during pregnancy.
Whole-body protein turnover measured by leucine and glycine kinetics, is augmented in the second and third trimesters compared with first-trimester and pre-pregnancy rates.(2)
Egg
Estimation of the additional protein required during pregnancy was based on increased maintenance needs estimated by nitrogen balance and total body protein deposition estimated from potassium retention.
The total additional protein required was 0.5g/day during the first, 9.5g/day in the second and 22.0g/day during the third trimesters of pregnancy respectively. Given the minimal amount of changes during the first trimester, no increase in requirement was stipulated.
To cover the needs of all pregnant adolescents and adults, the RDA was set at twice the coefficient of variation (12%) in protein requirements or at 25g/day of additional protein.
Dietary Fats.
Arachidonic acid (ARA) concentrations in red blood cell phospholipids decrease during pregnancy. but whether this is a normal physiologic response to pregnancy or a reflection of dietary inadequacy of omega-6 fatty acids is uncertain.
Because of the lack of evidence for determining the requirement during pregnancy, the IOM recommended an adequate intake at the median linoleic intake of pregnant women in the United States 13 g/day for pregnant adolescents and adults.
Whereas, for Indians 200mg/day DHA for optimal adult health and fetal development.(3)
Fish Oil
Similarly, lower docosahexaenoic acid (DHA) Concentrations in plasma and red blood cells have been reported for pregnant women; however, it is uncertain whether this reflects declining DHA status.
Supplementation with fish oil during pregnancy can increase blood concentrations of DHA in the mother and newborn infant.
Dietary Carbohydrate.
To ensure the supply of glucose for the fetal brain and maternal brain, the estimated average requirement for available carbohydrate was same as non-pregnant women (100 g/day), plus the additional amount required during the third trimester (35g/day).
Brown Rice
To allow for individual variation the RDA for available carbohydrate was set at 175 g/day for pregnant adolescents and adults.(4)
Iron.
Insufficient dietary iron during pregnancy can result in Iron-deficiency anemia. Epidemiologic evidence demonstrates that maternal anemia is associated with higher mortality preterm delivery, low birth weight and increased perinatal infant mortality.
High hemoglobin concentrations at delivery also are associated with adverse outcomes of preterm birth, low birth weight, and fetal death.
High hemoglobin concentrations are a result of decreased plasma volume attributable to maternal hypertension and eclampsia.
Spinach
Such nutrition i.e. iron needs increase during pregnancy, even though menstruation does not occur and intestinal absorption of this mineral is enhanced.
Dietary iron requirement during pregnancy covers basal losses, deposition in fetal and maternal tissues, and expansion of hemoglobin concentrations. Basal losses are estimated to be 250 mg over the 220 days of pregnancy.
Approximately 315 mg of iron is deposited in fetal and placental tissues, and the expansion of hemoglobin concentration accounts for 500 mg. accounting for individual variability and an efficiency of absorption of 25%, the RDA was set 38 mg/day.
When therapeutic amounts of iron (>30 mg/day) are given to treat anemia, supplementation with approximately 15 mg of zinc and 2 mg of copper is recommended, because the iron may interfere with the absorption and utilization of these trace elements.(5)
Calcium is required not only bone mineralization but also for vascular contraction and vasodilation, muscle contraction, nerve transmission, and glandular secretion. During pregnancy, the fetus accretes approximately 25 to 30mg of calcium, with maximum accretion rates in the third trimester.
Calcium absorption and urinary calcium excretion increase by approximately twofold in pregnant women.
Milk
Bone resorption as well as bone formation are increased during pregnancy, as reflected in the 50% to 200% to increase in bone turnover markers.
Total serum calcium concentration decreases, with a slight increase at term. These changes in calcium homeostasis are mediated part by the increase in calcitropic hormone1,25-dihydroxyvitamin D.
The physiological adaptation to meet the increased calcium requirement of pregnancy is the increased efficiency of calcium absorption.(6)
The recommended intake or adequate intake of calcium during pregnancy is 1300 mg/day for adolescents 14 to 18 years of age and 1000 mg/day for women 19 to 50 years of ages.
Zinc.
Zinc is vital nutrition during pregnancy which is essential for structural integrity of proteins and regulation of gene expression.
The additional zinc requirement during pregnancy reflects zinc accretion in newly synthesized maternal and fetal tissues.
Changes in intestinal zinc absorption appear to be the primary homeostatic adjustment in Zinc metabolism, to meet the increased demand for zinc. But this has been technically difficult to prove in women.(7)
Zinc
On the basis of maternal and accumulation of 2.7 mg/day and a fractional absorption of 27%, the RDA for zinc during pregnancy was set at 14.2 mg/day for adolescents 14 to 18 years of age and 14.5 mg/day for women.
Factors that interfere with absorption (i.e., high dietary phytate, fiber, and calcium; high doses of supplemental iron; gastrointestinal diseases) or placental of zinc (i.e., smoking, alcohol abuse, and an acute stress response to stress or infection) can cause a secondary zinc deficiency.
Pregnant women with these conditions may benefit from a Zinc supplement providing approximately 14.5 mg/day.
Iodine.
It is an essential constituent the thyroid hormones- thyroxine and triiodothyronine which regulate essential enzymatic and metabolic processes. Iodine deficiency results in delayed growth and development, mental retardation, hypothyroidism, goiter, and cretinism.
Goiter is the earliest clinical manifestation of iodine deficiency during pregnancy. Serum thyroglobulin and thyroid-stimulating hormone concentrations also increase.(8)
Salt
The daily accumulation of Iodine by the newborn Infant is estimated to be 100µg/day, with close to dally turnover. From studies conducted in iodine-deficient areas, it is estimated that 160µg/day prevented goiter in pregnant women.
Accounting for individual variability the RDA for pregnancy was set at 250 µg/day to prevent goiter in most pregnant women.
Vitamins.
Vitamin A is essential for normal vision, gene expression, reproduction, embryonic development, growth and immune function. Vitamin A deficiency in pregnancy is associated with preterm birth, IUGR, and low birth weight.(9)
Papaya
The RDAs for vitamin A during pregnancy of 750 µg/day for adolescents 14 to 18years of age and 770 µg/day for 19 to 50yrs of age are based on the accumulation of vitamin A in the fetal liver and on the assumption that the liver contains half the body’s vitamin A. Whereas, for Indians the RDA of vitamin A is 900 µg/day.
Folate.
Folate functions as a coenzyme in single-carbon transfer reactions involved in nucleic and amino acid metabolism. The term folate includes synthetic folic acid in fortified foods and dietary supplements and naturally occurring forms in food.
Therefore, the RDA was set at 300µg/day or 600µg/day of dietary folate equivalents. RDA of folate for Indians are 570 µg/day.
Women should be advised not to attempt to achieve 4000 µg dose from over-the-counter because of the risk of ingesting harmful amounts of other vitamins.
Also, the patient should understand that folate supplementation did not prevent all neural tube defects in clinical trials. Therefore, prenatal neural tube defect testing should still be considered.(10)
Vitamin C.
Vitamin C functions as an antioxidant and cofactor for enzymes involved in the biosynthesis of collagen, carnitine, and neurotransmitters.
Plasma concentrations of vitamin C decrease with the progression of pregnancy, probably as a result of hemodilution. The placenta takes up the oxidized form of ascorbic acid and delivers the simple form to the fetus.
Vitamin C deficiency is associated with increased risk of infections, preterm rupture of membranes, preterm birth and eclampsia.
The fetus is subject to maternal status, as evidenced by lower amniotic fluid concentrations of vitamin C in pregnant smokers than in non-smokers.(11)
Lemon
The RDA for Vitamin C is increased by 10 mg/day to allow for adequate fetal transfer. Higher amounts are recommended for women who use illicit drugs, cigarettes, alcohol and aspirin regularly.
Although there is no firm evidence of vitamin C toxicity during pregnancy. However, mega doses can result in high concentrations in the fetus, with possible induction of fetal hemolysis and oxidative damage in preterm infants. RDA of vitamin C for Indian pregnant woman is 65+15 mg/day.
Vitamin E functions as an antioxidant that prevents propagation of lipid peroxidation. Plasma concentrations of vitamin E increase during pregnancy along with total lipids.
Placental transfer of vitamin E appears to be relatively throughout pregnancy. Neither vitamin E nor toxicity has been reported in pregnant women.
There is no evidence that maternal supplementation prevents hemolytic anemia in preterm infants. The RDA for pregnancy is assumed to be same as that for nonpregnant women.(12)
Vitamin Supplementation.
A varied diet in accordance with the US dietary guidelines can meet all vitamin and nutrition needs associated with pregnancy; however, women whose dietary practices seem to be less than satisfactory may benefit from a prenatal vitamin supplement.
Special circumstances in which specific supplements are recommended includes:
Vitamin D: 10 µg(400 IU) daily is recommended for complete vegetarians (those who consume no animal products) and others with a low intake of vitamin D fortified milk; vitamin D status is a special concern for women at northern latitudes in winter and for others with minimal exposure to sunlight and, thus, at risk of reduced synthesis of vitamin D in the skin.(13)
Vitamin B12: 20 µg daily is recommended for complete vegetarians.(14)
Vitamin B6: Supplements of vitamin B, may prevent nausea and vomiting in early pregnancy, because vitamin B catalyzes a number of reactions involving neurotransmitter production. In 1991, results of a randomized, double-blind, placebo-controlled study were reported, in which vitamin supplementation was evaluated for its effect on nausea and vomiting in early pregnancy.(15)
Alcohol.
Consumption of alcohol adversely affects fetal development. Fetal alcohol syndrome is estimated to occur in approximately 1 to 2 infants per 1000 live births in United State.
More moderate drinkers may produce offspring fetal alcohol effects, such women also demonstrate a higher rate spontaneous abortion, abruptio placentae, and having infants with low birth weight.(16)
Beer
All women planning for conception should be advised to avoid consumption of alcoholic beverages.
Women with a known addiction to alcohol should be encouraged to enroll in a treatment program and practice contraception if treatment is unsuccessful.
Rehabilitation of women who are addicted to alcohol after conception may not prevent adverse embryonic development, but it may positively affect the growth of the fetus.
Caffeine.
The effect of caffeine as a nutrition on the course and outcome of pregnancy is still controversial.
Research using animals indicates that excessive amounts caffeine intake increase the incidence of congenital malformations; the effects of consuming smaller quantities (eg, 3 to 5 cups of coffee per day) have not been satisfactorily studied.
Coffee
Human observational data suggested that excessive caffeine intake is associated with an increased risk of miscarriage, even accounting for concurrent smoking.
Thus, common sense should prevail, and women, considering pregnancy could legitimately be advised to use caffeine in moderation if they choose to use it at all.(17)
Metabolic Disorders.
Discussing existing metabolic disorders may be critical to the health of both mother and infant. Examples of disorders for which early intervention is effective are maternal phenylketonuria and type I diabetes mellitus.
Metabolic control of both diseases involves conscientious dietary manipulation well before the critical period of embryonic development.
In the case of the woman with phenylketonuria, restriction of dietary phenylalanine is mandatory while satisfying the protein and other requirements of nutrition of mother and fetus during pregnancy.
The woman with Type 1 diabetes mellitus must control blood glucose concentrations through careful food selection and scheduled meal timing in concert with the administration of insulin.
By doing so, the risk of spontaneous abortion and congenital defects in the offspring can be markedly reduced.
Additional Nutrition and Lifestyle Concerns During Pregnancy.
Food Cravings and Aversions.
Most women change diets during the course of pregnancy. Some changes are based on medical advice, others on folk medical beliefs, and others on changes in preference and appetite that may be idiosyncratic or culturally patterned and should be aware that culturally sanctioned changes in diet may affect a woman’s willingness to follow prescribed dietary regimens.
The most commonly avoided foods during pregnancy are also excellent sources of animal protein: milk, meats, pork, and liver.
Cravings and aversions are powerful urges towards or away foods including foods about which women experience no unusual attitudes outside of pregnancy. The most commonly reported craved foods are sweets and dairy products.
The most commonly reported aversions are alcohol, caffeinated drinks, and meats. However, cravings and aversion are not limited to any particular foods or food groups.
Herbal Teas.
Pregnant women should be discouraged from unlimited consumption of herbal teas, because the composition and safety of most herbal are unknown.
Rather than seek approval from the US Food and Drug Administration, most manufacturers of herbal tea preparations stopped marketing the mixtures as medicine and simply list the ingredients on the label.
Because of lack of safety testing, pregnant women should be cautious herbal tea mixtures. They should be advised to choose only products in filtered tea bags and to avoid displacing more nutritious beverages, to limit herbal tea consumption to 2 servings of 8 oz per day.
Food Additives and Contaminants.
The teratogenicity of specific common food additives would be a major concern if the US Food and Drug Administration did not require animal testing of new additives for their potential to cause birth defects. Some food contaminants are recognized as harmful to a developing fetus.
Exercise During Pregnancy.
It is important to get the right information about exercise and nutrition during pregnancy. However, along with the nutrition it is also very important to perform some physical exercise during pregnancy.
In the absence of medical or obstetric complications, pregnant women who engage in a moderate level of physical activity can maintain cardiovascular and muscular fitness throughout the pregnancy.
Yoga
In the absence of either medical or of obstetric complications, 30 minutes or more of moderate exercise a day. Women with GDM may benefit from exercise.
Bottom Line.
Last but not the least, it is very important to plan a balanced nutrition during pregnancy. Your diet must contains all above mentioned minerals and vitamins which support the growth of the baby.
However, a light exercise is also plays an important role during pregnancy. So, it is recommended to lead a healthy life with a healthy nutrition.
+17 Sources
Freaktofit has strict sourcing guidelines and relies on peer-reviewed studies, educational research institutes, and medical organizations. We avoid using tertiary references. You can learn more about how we ensure our content is accurate and up-to-date by reading our editorial policy.
Our team of experts is always monitoring the health and wellness field,
ensuring that our articles are updated promptly as new information emerges.
See Our Editorial Process
Current Version Mar 19, 2026
Written By: Nebadita
Reviewed By: Jennifer Roelands
May 16, 2021
Written By: Nebadita
Reviewed By: Jennifer Roelands
The dietary recommendations provided here are based on research and expert review. Individual needs vary — please consult a registered dietitian or nutritionist before changing your diet.
Know More
Nebadita is experienced in the field of nutrition, health, fitness, and more. Nebadita earned Master Degree from National Institute of Nutrition, Hyderabad and currently serving in the Eastern branch of ICMR. Know More.
Learn about our editorial process..
This content is based on scientific research and written by experts.
Our team of licensed health professionals, nutritionists and fitness experts endeavor to be unbiased, objective, honest and to present each sides of the argument.
This article contains scientific references. The numbers in the parentheses (1,2,3) are clickable links to peer-reviewed scientific researches.
Our Review Process
FreakToFit’s articles are reviewed by board-certified physicians, nutritionist and fitness professionals. Medical Reviewers confirm the article is in-depth and accurate, reflecting the latest evidence-based research. Article is reviewed before publication and upon significant updates. Learn more.
Jennifer Roelands, MD
Jennifer Roelands, MD, is an integrative remedy skilled OB/GYN with 18 years of experience. She is the founder and director of Well Woman MD, which affords complete fitness care for ladies.










































 Workout
Workout

 Meditation
Meditation



 Podcast
Podcast
 E-book
E-book