







































 Workout
Workout

 Meditation
Meditation






 Podcast
Podcast
 E-book
E-book



GLP-1 medication (semaglutide, tirzepatide and analogs) is reliable in decreasing the appetite and the weight, although some individuals lose a greater proportion of lean body mass than anticipated.
A targeted resistance-training program and sufficient protein and savvy nutrition, progressive overload, and frequent monitoring are the surest methods of safeguarding muscle when on a GLP-1.(1)
The following will provide latest evidence and ready-to-use programs (beginner to advanced) examples of microcycles, protein goals, tempo/volume suggestions, cardio, and trouble shooting.
Related Stories
 Curtsy Lunges Exercise: Benefits, Steps and Precaution
Curtsy Lunges Exercise: Benefits, Steps and Precaution
 Best 10 Kettlebell Exercises for Glutes: Get a Lifted and Toned Butt
Best 10 Kettlebell Exercises for Glutes: Get a Lifted and Toned Butt
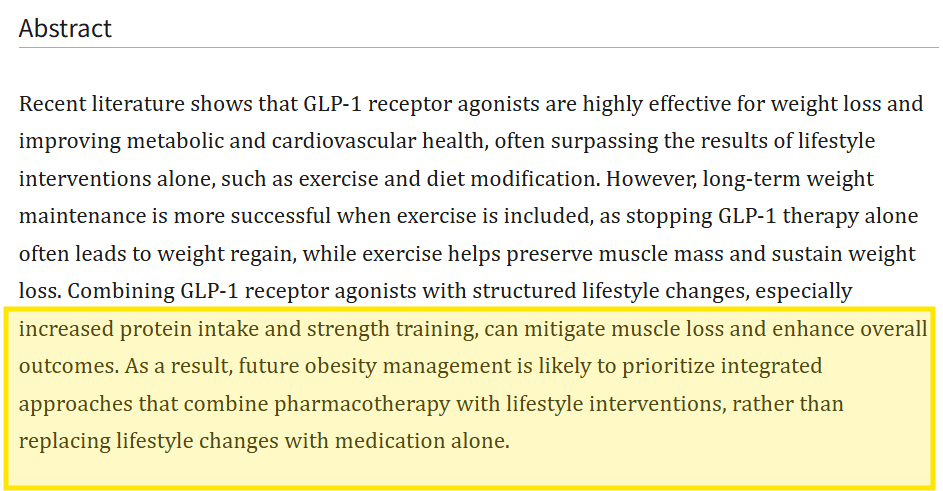
Recent reviews and trials indicate that exercise + protein can maintain to a great extent lean mass in case of pharmacologic weight loss.
The reason muscle is important on GLP-1s and what the evidence tells us.
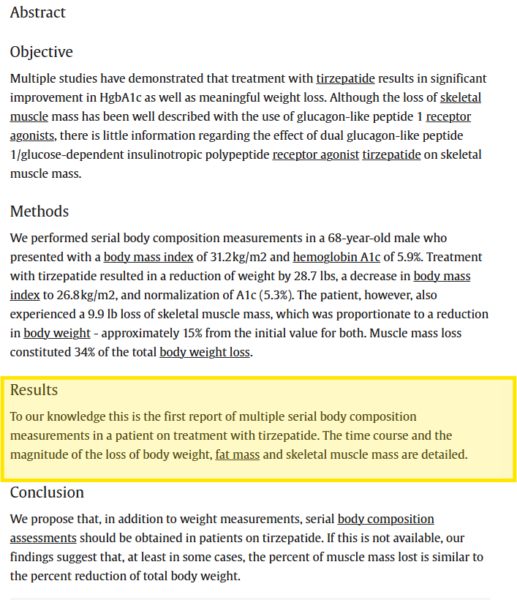
GLP-1 receptor agonists and dual agonists (e.g., tirzepatide) have a massive effect on fat loss in most individuals – but due to a proportional reduction in total body mass, the lean mass (including skeletal muscle) also tends to decrease.
Individual reports and analyses indicate a significant skeletal muscle loss in a small proportion of patients. That is not mere cosmetic: the loss in muscles can decrease the strength, mobility, metabolism, and long-term functional health. Recent reviews and subsequent preliminary clinical data indicate that this lean mass loss can be significantly blunted or prevented by organized resistance training and maintenance of high levels of protein intake.(2)
It is noteworthy that larger datasets continue to emerge and findings differ according to age, baseline muscle mass, and rate of weight loss, and also include the inclusion of resistance training in the lifestyle support in trial.
Other more recent studies even indicate a maintained strength despite a small decrease in lean mass, suggesting that function and mass do not decline in the same proportion. Nonetheless – the best bet would be strength training on the offensive.
The essence strategy.
Focus more on heavy-ish resistance training (progressive overload, 2-5 sessions/week, based on experience) – it is the most important behavior to maintain/build muscle.
Consume adequate protein of good quality that is spread throughout the day. Protein + resistance training has the greatest impact on muscle retention.(3)

Monitor and adjust – keep an eye on strength, you can do things by time (e.g. timed sit-to-stand), body composition (in case possible), but reduce weight loss when the strength is declining, and you are losing a significant amount of lean tissue. Combined interventions (resistance + additional protein) to GLP-1 patients are being trialed.

Who should be extra careful?
- Age-associated sarcopenia (40 and above).
- Extremely low mass or weakness of muscle on base.
- Very high weight loss (greater risk of proportional lean mass loss).
- Individuals that are limited in mobility or have chronic disease- adapt programs and consult clinicians.
- Whether you belong to one of those categories, you need to rely more on the frequency of resistance training, protein targets, and you might need to employ the services of a physiotherapist or certified instructor.
Nutrition that is vital in muscle maintenance on GLP-1s.
- Protein goal: 1.2-2.0 grams of body weight per day in about 0.5kg/day body weight (higher target in older, extremely active or rapidly losing weight). The number of experts suggests 1.62.2 g/kg/kg of fat-free mass as the optimal percentage of preservation/gain in energy restriction. Evenly divide protein (20 -40 g) into 3-4 meals.
- Calorie plan: In case you are prescribed calorie restriction by your physician using GLP-1, do not use extreme deficits. The less rigorous deficit (300-500 kcal/day) with resistance training is more likely to spare more muscle compared to the very violent dieting.
- Leucine dosing schedule: Targets: 2.5-3g leucine/protein meal (whey, dairy, eggs, soy isolates aid). Protein after exercise in 1-2 hours is also beneficial but not compulsory in case daily protein is obtained.
- Supplements (optional): Creatine monohydrate (3 to 5g/day) is supported by a considerable amount of evidence to aid in achieving strength and lean mass increases in conjunction with resistance training. Vitamin D if deficient. Take supplements under the doctor.
- Hydration & GI: GLP-1s may lead to reduced appetite and, at the initial stages, may induce nausea, so it is better to choose small frequent protein foods (e.g., Greek yogurt, protein shake) in case of intolerability of large meals.
- Combined resistance + protein strategies: (which are specifically tested in GLP-1 users) are in clinical trials (with positive early results).
The question is how to develop a resistance program that will keep muscle.
Principles to follow:
- Progressive overload: Add weight, reps or sets. Track lifts.
- Big systemic advantage of multi-joint lifts first: Squat/hinge/push/pull lifts.
- Volume and intensity: To maintain or increase throughout weight loss, do 8-20 hard sets per major group of muscles per week (less when starting out, more when more experienced). Hypertrophy Use 6 -12 rep range and strength Use 3 -6 rep range, occasionally.
- Frequency: Exercise each muscle group 2-3 times a week in the majority of people; divide the routine in case of high frequency.
- Speed / loading: Control Eccentrics can be used to maintain muscle with calorie intake. Lowering phases of 2-4 seconds can be useful.
- Periodization: Fluctuate between heavier strength blocks and higher volume hypertrophy blocks every month to prevent plateaus.
- Recovery: The program includes sleep, protein, and rest days; GLP-1s do not alter the recovery principles – recovery is necessary.
Ready-made programs (whichever one and follow it during 8-12 weeks).
Note: scale loads to ensure final 1-2 reps of a set are similar to the first ones but difficult but with proper form.
Warm up: Before every session, warm-up 5-10 minutes.
1) Beginner (0–6 months training) — 3 days/week Full-Body (ideal for new lifters).
Goals: Develop neural properties and establish muscle mass.
Weekly layout: Mon / Wed / Fri.
Each session:
- Squat variation (bodyweight/ goblet/ barbell back squat): 3 x 8-12.
- Push (push-ups to dumbbell bench press): 3 × 812.
- Hinge (Romanian deadlift or kettlebell swing): 3 x 8 -12.
- Row (single-arm dumbbell row or seated cable): 3 x 8 -12.
- Overhead press (DB or barbell): 2 × 8–12.
- Core/hip (3 plancks 30 -60s or glute bridges 12).
Progression: Each time add 1-2 reps in each set till you are going to the top of the range, add weight. Increase weight on main lifts by +5-10 percent in every 2-3 weeks.
2) Intermediate — 4 days/week Upper/Lower split.
Goal: More volume per muscle group to preserve mass during caloric deficit.
Weekly layout: Mon (Upper A), Tue (Lower A), Thu (Upper B), Fri (Lower B).
- Upper (A): Bench press 4×6–8; Bent-over row 4×6–8; Incline DB press 3×8–10; Pull-ups/lat pulldown 3×8–10; Face pulls 3×12.
- Lower (A): Back squat 4×6–8; Romanian deadlift 3×8; Bulgarian split squat 3×8–10 each; Calf raise 3×12.
- Upper (B): Overhead press 4×6–8; DB row 4×8–10; Chest fly 3×10–12; Chin-ups 3×max; Triceps 3×10.
- Lower (B): Deadlift 3×4–6 (heavy); Front squat 3×6–8; Hamstring curl 3×10; Farmers carry 3×30–60s.
Progression: Track weekly; increase load or reps, keep 1–2 top sets heavy.
3) Advanced — 5 days/week (bodybuilding + strength hybrid).
Goal: Maximum muscle retention/gain while losing fat with GLP-1. Use only if you have lifting background and recovery capacity.
Structure: Push / Pull / Legs / Upper accessory / Lower accessory or similar. Weekly volume per muscle: 12–20 sets.
Include one heavy strength day (3–6 reps), one hypertrophy day (8–12 reps), and one metabolic conditioning day (short circuits) weekly. Prioritize sleep, protein, and auto-regulate (drop volume when fatigued).
Cardio: what to do (and what not to do).
- Maintain some cardiovascular to keep the heart healthy and add to the calorie expenditure but not too much long and steady-state cardiovascular since this may enhance muscle loss when nutrition and training are insufficient. two or three 20-30 minute moderate sessions in a week suffice.
- Include HIIT with caution (1 -2 sessions/week) in case you can tolerate it – does not necessarily damage muscle in case strength training and protein are adequate.
- It is better to walk/cycle early in the morning (low impact) when GLP-1 makes you feel dizzy/nauseous.
Sample 7-day microcycle (intermediate).
- Mon: Upper A (heavy) + 15 min walk
- Tue: Lower A (strength focus) + mobility
- Wed: 20–30 min easy bike + core
- Thu: Upper B (hypertrophy)
- Fri: Lower B (hypertrophy) + short conditioning (10 min sled/row)
- Sat: Active recovery walk/yoga
- Sun: Rest + flexibility
Monitoring: how to be sure that your program is working.
Strength trends: When your major lifts are steady or rising positively then this is a good sign. Weakness progressing ↓ Evaluate calories, protein, and rest.
Functional parameters: Sit-to-stand time, stair test, or ADL.
Body composition: In case of availability, DEXA/BIA is carried out after every 8-12 weeks. Observe mass loss as compared to fat loss. Randomized studies of GLP-1 in the absence of exercise in the early years have occasionally observed comparative lean mass decreases. Response to that by adding resistance training.
Symptoms: excessive fatigue or dizziness or constant weakness, inform clinician.
Real life (GLP-1 side effects, appetite loss, and training) tips and tricks.
- Nausea or loss of appetite: take protein shakes in a liquid form, made up of blended food, and plan training at the time when you feel least nauseous. Large amounts of protein can be provided in small concentrated meals.
- Energy dips: the warm-ups can be shorter and the range of rep can be slightly lower (heavy, fewer reps), which is more comfortable than long high-rep sets with a low level of energy.
- Timing of medication: there are those who train at times when medication effect is stable; ask your prescriber to give you specifics of this.
- Track protein initially: Precision in calories, as opposed to muscle retention by hitting protein targets, is lesser when on GLP-1s.
Special population notes.
- Elderly: Focus more on resistance (within the limits of safety), balance, and increased protein (nearer to 1.620g/kg). Take into consideration controlled programs.
- Diabetics: GLP-1s have frequently been used in the management of diabetes. Check blood sugar levels prior to and following exercise; seek medical advice on how to alter the dosage of insulin/medications.
- Pregnancy/ lactation: GLP-1s are contraindicated; the professionals should design training programs.
Top pitfalls in programs and their solutions.
- Pitfall: How not to lift heavy enough.
Fix: Intend to get not less than a set per class of muscles per exercise that is close to failure (2 reps short). Intensity should be gradually increased. - Pitfall: Protein too low.
Fix: Eat more protein at breakfast/lunch/dinner and a post-workout snack- shake can be used in case of low appetite. - Pitfall: Overdoing cardio.
Fix: Cut cardio during heavy training blocks or when losing strength; substitute with low impact activity. - Pitfall: No progressive plan.
Fix: Simple progressions +1,2 reps +2.5,5 percent load +shorter rest period of conditioning.
The future of research and its importance.
There is ongoing clinical research to determine whether or not structured resistance training and increased protein has the ability to reliably maintain lean mass in GLP-1 therapy.
The combination approaches have been shown effective in early 2020s papers and reviews, and the ongoing studies (and discontinued/altered trials) suggest that the medical community is concerned with muscle maintenance during pharmaceutical weight loss.
It implies that there will be better standards and more subtle suggestions in the years to come, however, at present, the powerful prescription that dominates is: lift heavy, eat protein, monitor.
Note: pharmaceutical researchers are trying to develop GLP-1s with muscle-preserving drugs, although there is no certainty about results or availability.
To illustrate, the recent clinical trial of bimagrumab (a proposed muscle-targeting drug) in combination with tirzepatide was discontinued due to business considerations, which underscores the need of muscle-sparing agents, as well as the difficulty of creating them.
Quick 30-day starter plan (action checklist).
- Pick a program above (beginner/intermediate).
- Log initial lifts (1–5RM approximations) and body weight.
- Aim for 1.4 g/kg/day protein as a baseline — adjust upward if older/active.
- Train resistance 3×/week minimum; each major muscle group 2×/week.
- Add creatine 5 g/day if no contraindications.
- Reassess strength and energy after 4 weeks; adjust volume or food.
- Book a DEXA/BIA if you want precise lean mass tracking (every 8–12 weeks).
Frequently Asked Questions.
1. Will GLP-1s result in muscle loss?
Not always. The loss of mass is usually common yet unpredictable; the structured resistance training, along with protein, significantly decreases such a risk.
2. Can I still do cardio?
Yes – moderate cardio, but not very high volumes, in case of loss of strength.
3. What is the quickest that I can anticipate changes?
Strength gets stable after 4-8 weeks provided that you train and consume protein. The changes in body composition can be monitored after every 8-12 weeks.
Bottom Line.
Provided you are using a GLP-1 and want to preserve muscle, embrace a progressive resistance-training regimen (3x/week starting 4/5 x/week), reach ~1.2- 2.0 gram/kg protein/day distributed evenly, creatine, and performance and activity.
Most individuals can gain significant muscle mass and maintain strength with this combination and the data is increasing that exercise + protein is the most effective real-life intervention as these drugs take over their task.
+3 Sources
FreakToFit has strict sourcing guidelines and relies on peer-reviewed studies, educational research institutes, and medical organizations. We avoid using tertiary references. You can learn more about how we ensure our content is accurate and up-to-date by reading our editorial policy.
- GLP-1 agonists and exercise: the future of lifestyle prioritization; https://pmc.ncbi.nlm.nih.gov/articles/PMC12683586/
- Skeletal Muscle Mass and Body Weight Fall Proportionally With Use of Dual Glucagon-Like Peptide 1/Glucose-Dependent Insulinotropic Polypeptide Receptor Agonist Tirzepatide: Case Report and Review of Literature; https://www.sciencedirect.com/science/article/pii/S2376060524001378
- Preservation of lean soft tissue during weight loss induced by GLP-1 and GLP-1/GIP receptor agonists: A case series; https://pmc.ncbi.nlm.nih.gov/articles/PMC12536186/













